
by Assunta Ginanneschi
They are called “rare diseases”, but experience shows they are not that rare at all!
Personally, I know at least three people affected by rare diseases. In fact, on average, one of every 10 to 12 people you know has a rare disease. As Jessie J might say, “Nobody’s perfect”.
Which is to say, everybody has some peculiarity, or if you wish, everybody is rare!
This blog post will concern favism, also known as glucose-6-phosphate dehydrogenase deficiency (G6PD deficiency). Let’s start with the story of my good friend Luca T.* I still remember his wedding…what a wonderful day!
Receiving His Diagnosis / Discovering His Condition
Luca T. was diagnosed with favism during his military service. Generally the diagnosis, for this disease and so many others, is done via accurate blood tests or DNA testing.
The favism test was at that time still a routine procedure in the Italian army. The corporal called his number in front of the whole base and yelled something like ”Who is number 135? You have favism”.
He asked “What’s that?” and one of his comrades tried to explain, “This means that you’re too much like a fava bean!” Well, take it as a compliment, Luca T.!
Actually the disease is a bit more complex than that: when exposed to fava beans, the affected individual will experience severe episodes of hemolytic anemia (favism), where red blood cells self-destruct and set off a chain reaction of debilitating symptoms.
G6PD deficiency or favism is an X-linked recessive trait. Therefore, symptomatic patients are mostly males.
The G6PD deficiency is the most common human enzyme defect, being present in more than 400 million people worldwide. African, Middle Eastern, Mediterranean and South Asian people are affected the most, including those who have these ancestries, which is why it was a standard test for the Italian military.
This video explains the importance of being aware if you may be affected.
Treatment and Outlook
There is no specific drug for favism. People with favism must avoid known triggers like: viral infections, some drugs like antimalarials and analgesics, specific foods, most notably broad beans and certain chemicals (e.g. oxidants).

Because favism is a rare disease, much is unknown and many open questions are still on the table. These include:
- How is possible to stop or prevent the hemolytic crisis if the patient comes in contact with the triggers?
- Which are the first aid measures?
- Can the Glucose-6-phosphate dehydrogenase deficiency be corrected by an API supplement (e.g .Liposomal Glutathione) or external enzyme administration? Some work on glutathione-elevating compositions has been done on this question. (Glutathione-elevating compositions and uses thereof WO2014016831A1)
- Which drug delivery form would be more suitable for this purpose?
Moreover, new medical advance may mean new alternatives for favism and all rare diseases. There is news coming out every day.
It may be that the stem cells approach offers a definitive solution to the problem.
Other research could help predict limitations or complications are foreseeable in humans.
Advocacy:
The Italian Government plans to revoke the ”rare disease” designation for G6PD-deficiency. This means that neo-natal screening will be no longer obligatory and treatment expenses will not be paid by the healthcare system. There is a petition currently running on change.org for defending the patients’ position.
Such petitions raise the questions of how much it costs cover the yearly treatment expenses for a rare disease, and who should cover them? Is there any EU or international guideline concerning rare disease designation? Should there be?
As Luca can attest, it is important to screen for this disease if you are a potential carrier, as many Mediterraneans are. Please sign to raise awareness about favism!
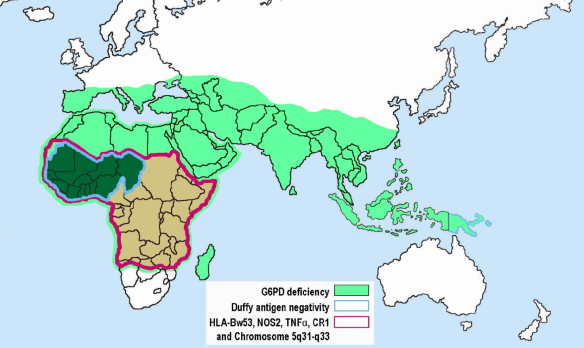
Connection to Malaria
There’s another reason to keep favism in the spotlight. Apparently G6PDD is protective with respect to P falciparum (and possibly P. vivax) malaria. This can be explained after the evolution theory: the genetic modifications occur random and the environment selects for those modifications that are advantageous for that context. One possible advantage is that cells infected with the Plasmodium parasite are cleared more rapidly by the spleen. This clue comes from looking at population distribution: favism tends to appear in past and current endemic malarial areas.
Historical distribution of malaria

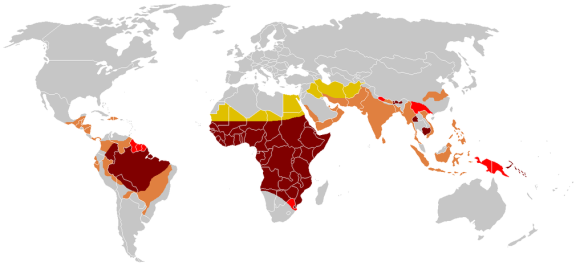
Modern distribution of malaria
So favism may be the body’s way of preventing malaria! In 2007, an article on Glucose-6-Phosphate Dehydrogenase Deficiency and Antimalarial Drug Development tried to connect the two diseases.
Is there any anti-malarial drug now that uses this strategy?
Then: is it medically and economically sustainable to keep the favism among the rare diseases? The potential link between a rare disease, favism, and a deadly, widespread, but neglected, disease, malaria, would be worth investing additional resources to solve both problems.
We have already contacted some malaria researchers in order to find out how this enzyme can be useful for finding new therapies. We’ll update this post as soon as we have new info.
*Name changed to protect the patient identity against sensitive data exploitation.
References:
Glucose-6-phosphate dehydrogenase deficiency, Genetic home references, a service of the U.S. National Library of Medicine®
Glucose-6-Phosphate Dehydrogenase Deficiency, NORD, National Organization for Rare Diseases

There are a lot of inaccuracies in this blog post. To name a few:
There is no such thing as a G6PDD carrier and G6PDD is not recessive. Everyone with an affected X chromosome reacts to triggers to some extent. This was proven by two separate research groups in 1962, but some myths die a hard death.
There are actually more women with G6PDD than men.
So called Favism reacts to much more than just fava beans.
All reactions do not result in a crises. In fact most G6PDD reactions to triggers are undetectable but can cause a lot of serious health issues over time.
LikeLike
Thanks for your feedback and continuing work to raise favaism awareness, Dale! As you no doubt are aware, rare diseases are often underfunded, and keeping up with the latest information is a challenge…but that’s why we’re here!
We have to be careful about replies whose goal seems to be to redirect traffic to other sites, but we take your concerns seriously and stand by our post.
According to The National Library of Medicine at the National Institutes of Health, G6PDD is indeed linked to a recessive X gene, and is more prevalent among men.
We never assert that favism reacts only to fava beans. Our actual quote above is: “People with favism must avoid known triggers like: viral infections, some drugs like antimalarials and analgesics, specific foods, most notably broad beans.” Neither have we maintained that all exposure leads to crisis. Indeed, we strongly advocate for continued standard testing among populations in which the condition is more prevalent, as exemplified by our link to the petition to retain the rare disease designation in Italy. Testing is vital even prior to the onset of symptoms!
We hope this clears things up! Thanks again for taking the time to write!
LikeLike
Pingback: Rare Disease Day: Get to Know Rare Disorders & Manage Them Better | CheckOrphan